Hi guys,
Forgot to let you know but I've moved. So if you still want to read my blurp then head over to my WordPress page.

Mostly random writings about healthcare and music stuff. This blog will be updated on a very strict "As and When it pleases me" schedule.
Tuesday, 6 November 2018

Friday, 15 June 2018
Metal Nurse: Acquired Brain Injury

So what exactly is ABI?
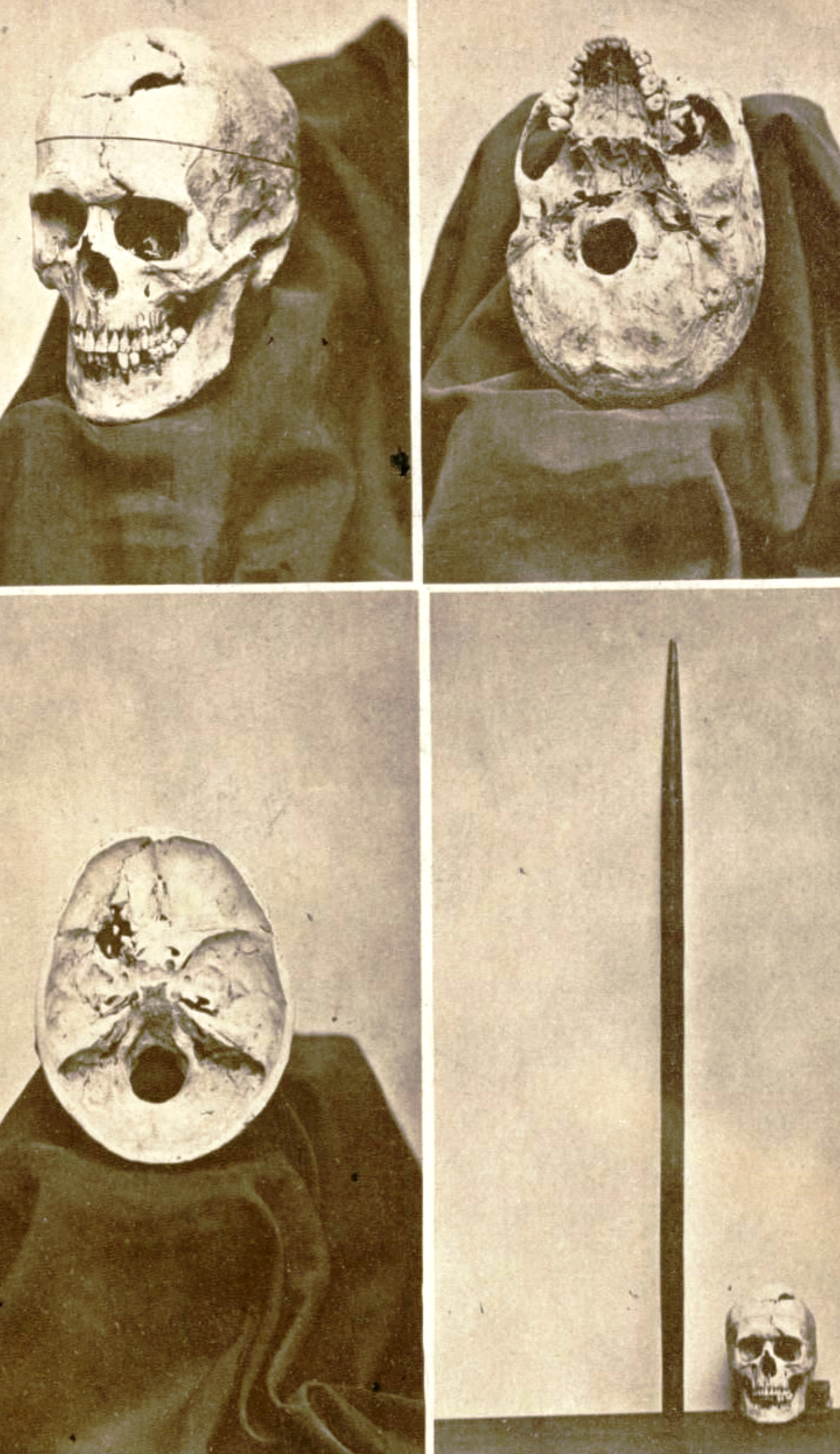 |
| Gage's skull and the iron rod |
 |
| Helmets prevent ABI |
What are the effects of ABI?
 |
| Brain MRI. |
"Aphasia is an impairment of language, affecting the production or comprehension of speech and the ability to read or write."This inability to be able to say what you mean to say, or form the right words, or sentences, can become very frustrating for the patient. And their closest. It can have a major impact on their rehabilitation and recovery.
There is also Ataxia, which according to the Ataxia UK,
"Ataxia’ is an umbrella term for a group of neurological disorders that affect balance, coordination and speech. There are many different types of ataxia that affect people in different ways. "One of the more challenging aspects of these patients care in my view is something called "Cognitive Fatigue". This is where a patient gets more tired and has greater difficulty in concentrating on things that they used to be able to do with ease prior to their injury. This can lead to fluctuation in their mood and difficulties with their emotions and behaviour. Thankfully with the right support, and right support network this can be overcome through intensive rehabilitation.

- tonic-clonic seizures, also known as grand mal.
- focal seizures
- Absences seizures
- Atonic seizures, also known as drop attacks
These seizures can be short and only happen once, or they can be long and come upon in groups. Typically these are brought upon due to external triggers, such as flickering lights, environmental noises, poor diet (for example badly managed diabetes or excessive amount of stimulants like caffeine and sugar) etc. But with patients who have ABI, they more often occur due to internal triggers such as lack of sleep, stress, emotional excitement and boredom. Those who have ABI tend to be put on anti-epileptic medication prophylactically in order to prevent them from having seizures. Most seizures tend to be self-terminating but carers and family need to have rescue medicines such as buccolam, which is an oral solution, or rectal diazepam in order to cut those seizures short, especially if the patient has had more than the one seizure. Then there is Status Epilepticus, this is a seizure that lasts for longer than five minutes. It is an emergency situation often requiring intensive care input. The prognosis for patients who suffer from status epilepticus is not good, between 10%-30% of those who are diagnosed with it die within a month. Hence the need for speedy treatment, with optimisation of their medications and daily routines, such as strict sleeping regimes.
As can be read this is a very big topic to write about, and there are issues that I have not touched upon. As I have mentioned frequently, this is a major global health concern. It has a multi-faceted impact. It does not just impact on the patient who suffers from the injury, it also affects their friends and family. But not just that due to the disability that comes with it and given the age it occurs most commonly, it can also affect the larger economy. The rehabilitation can take months if not years if they were in employment they will either have to take a long period off in order to return or never return at all. There is a definite need for more centres that provide rehabilitation and treatment for ABI, and this can only be beneficial to everyone. Not just those directly affected.
For further information, I wholeheartedly recommend an organization called Headway who dedicate themselves solely to those who are affected by head injuries.
Tuesday, 24 April 2018
Metal Nurse: Open visiting hours
 |
| Usual reaction |
Now. This is not going to be a popular opinion. But... I think that the above-mentioned hospital is correct in extending the visiting hours. Visitors do have their own lives to lead, their own needs that need to be met. So why do they have to organize their lives around those visiting hours? With those new hours, the visitors can come in dribs and drabs as opposed to coming in like a slow mowing gnu herd which makes everyone miserable. A patient with a large family can have one or two people visiting them throughout the day as opposed to having a whole tribe sat around the bed space, potentially annoying the rest of the patients and their visitors in that bay. Not to mention the issues with parking, which does seem to peak at visiting hours.
A lot of hospitals started giving relatives and friends of patients with relatives access to the ward outside normal visiting hours, after a campaign called 'John's Campaign' which has been extremely helpful to both patients and the professionals that take care of them. The thing is that more liberal visiting hours is better for patient care. You get fewer complaints, the patients get better quicker and they tend to be more settled during their stay. Patients satisfaction of their care improves. Which is always excellent. If visitors come in more infrequently this also gives nurses time to educate both the patient and their visitors, especially in terms of self-management and health promotion, which ideally should be part of all good care. Or it gives you enough time to figure out what happened, why it happened and how (hopefully) it can be prevented from happening again. Because collateral history can make such a big difference in patients care.
It is by no means perfect, but to be honest it doesn't have to be. We are there to try and make sure that the patient gets better. And opening the visiting hours does exactly that.
Sunday, 15 April 2018
Metal Nurse: Cancer quackery and the vultures that peddle them
These vultures need to be stopped.
One of the main points to keep in mind regarding cancer is that there are at least 100 different types of cancers known. Each with their own pathophysiology's, each with their own characteristics and each with different ways of treatment. So when you see someone that claims that they can cure cancer or know how. Ask them which type of cancer, then ask them how.
 |
| Chronicle Flask |
The body self-regulates its acid-alkaline level. The body maintains a very strict pH of 7.35 - 7.45. Go below that and you go into acidosis and go above that and you go into alkalosis. Both can and will kill you. A glass of lemon water is not going to do anything to shift it either way.
And honestly guys. The same goes for Bicarbonate of Soda. That excellent baking ingredient and cleaning material. The same doofuses who talk about cancer being acidic also advocate that people eat a whole load of Bicarb. You might neutralize you gastric acids for short period, and given the quantities, you would have to eat in order to do anything to cancer cells you would also neutralize your vital statistics.
 |
| XKCD: Cells |
I do have a lot of people on my FB friend list and a lot of them are well-meaning. But sometimes they share memes that are more harmful than helpful. I have seen a lot of people share memes and quackery articles that usually have something to do with 'XYZ kills cancer cells, scientismints prove!'. The problem with that is that ANYTHING will kill cancer cells in a petri dish, including washing up liquid. You are not going to cure cancer with washing up liquid. In vitro studies can be interesting, but sadly do not translate into the real complex systems like the human body. For example, a popular meme walks about cannabis killing cancer. Again at Cancer Research provides an excellent article laying out the truth regarding Cannabis, it uses in cancer treatment and what current evidence says about it. Cannabis has been found to be very useful in managing nausea, pain, anxiety and other side effects from the cancer treatment. But it is still not the cure for cancer.
Then there is this thing that cranks want to discuss called Vitamin B17. Can I just clear things up? There is no such thing as Vitamin B17. What these con people are referring to is a substance better known as amygdalin. Amygdalin is a perfectly natural compound which is found in apricot kernels, lima beans, clover, peach stones and many many more. When consumed amygdalin converts to cyanide. It is not a vitamin. It will kill you, I suppose in a way it does kill cancer.
What people sometimes have to bear in mind when they read miracle stories about cancer is the phrase Spontaneous Remission. Basically this is where cancer starts to improve for no discernible reason, it does happen. But it happens really, really seldom. Currently the statistics surrounding this is 1 in 100,000. If you know someone who this has happened to then be happy for them, but be vary of any talk about alternative therapies.
Saturday, 14 April 2018
Carpe, The Kings are dead, long live the kings.

From a purely musical perspective these guys were one of the most original composite bands I have had the pleasure of listening to. The mix of funk, jazz, hip hop, blues and hard rock with big band sentimentalities was all played with such confidence and relish. It could be argued that Flash is the front and centre of the band but that would be doing injustice to the rest of them because they all play such significant roles.
For example I remember seeing Carpe playing with Frenchie, the guitarist and singer, and they had to replace him with three other people. Jon Moore on lead guitar, is, well... Wow, those guitar solos were really rather awesome and never out of place. Frenchie's subtle rhythm guitar playing can't be underestimated, underpinning a lot of the songs. Has to be added that Flash is an excellent rapper, but they also have three really rather excellent singers who all have different styles but complement each other almost perfectly. Dave, Grum and Rachel's rhythm underpinning everything.
The thing that will stand out most is that what these guys wanted first and foremost was to have a good time and to make sure that everyone else did as well. I am going to miss knowing that they will be playing a gig locally.
Monday, 9 April 2018
Metal Nurse Sojourn: Part 3, Sofia and getting lost in the woods
 |
| Lost In The Woods |
The next day I got up early, got packed up, paid the hostel and set off to find that mysterious bus station again. In order to head back to Sofia. My other half had said that getting a bus was both quicker and cheaper, and of course provided better sightseeing opportunities than a train. Seeing as she had done a helluva lot more travelling than me, I took her word for it. She was correct. Getting the ticket was a bit of a trick, seeing as the lingua franca is Russian, but I did manage to obtain one. Then there was a bit of a misunderstanding regarding the seats, as I hadn't clocked on that that the seat numbers were on the tickets. Somehow I had expected it to be similar to the British system where people just plonk their butts anywhere. I got a mournful look from a Bulgarian grandmother and an international sign language explanation from another. The bus was full, and it was hot. And it only got hotter by the minute because the bus driver didn't want to open any windows or turn on the AC. It became very hard to keep my eyes open.
 |
| Hostel Mostel in Sofia |
After my kip, I go back to the common room of the hostel, get shown a map of where to go, where to eat and what there is to see. Then also with some aid from Google, off I trot.
 |
| Monument To The Soviet Army |
Oh and the monument, sadly scrubbed clean. Still nice and well done and fascinating to walk around and look at. Just not pop-culture referencing nice. So time to walk some more. Oooo, a squirrel... A BLACK SQUIRREL. That looks like a red one! Maybe we should import those into the UK. Oh, but it is the same species as the red one. Never mind then. Damn it was cute though.
The weather is still very nice so I just take my time to walk around the parks of Sofia. It is a nice city, good to spend a couple of days at. But to be honest, Plovdiv was nicer. Sofia is also slightly more expensive but that isn't really saying an awful lot. The one detail I did notice about Bulgaria is that there is not a lot of microbreweries. Which saddened me a little, there are some nice cheap lagers to be had. There was a lot of choice in vodkas and wines, but I prefer my ales. The city is alive, smells clean, and is not crowded with too many tourists. I know there are tourists around because the hostel is teeming with them. But it's not overrun with them like Prague. After much walking, I return back to my hostel to do some more writing and eat.
 |
| Sofia Day One |
 |
| National Museum of History |

I don't think I w
{kind=link}
ant to press my luck too much. But I did manage to get into the museum. Which was captivating, the history of Bulgaria is an intriguing hotchpotch of different cultures amalgamating together. The Greeks have been here, The Romans, The Thracians, Bulgarians, the Ottomans and many more. Invaded by Hungarians, Mongolians, Serbs, and many more still. Then of course as can be seen above they have had a lot of input from the Soviets. Then there is the history of the Cyrillic alphabet itself, which remains the only alphabet where we can trace it back to its original creator, Clement of Ohrid. After taking another moment to stop and have some coffee, I take in the view. Specifically, the mountain that Sofia is based right next to. I want to take a photo up there. So again after consulting with Google Maps (Even though it probably did try and get me killed before), I vacate the museum after spending a good two hours walking around. On my way out the guard eyes me up suspiciously with a cigarette in his mouth, doughnut at hand and a big gut. Probably feeling like he should be doing his job, he asked me to hand my bag over so he could search it. Thankfully I only had bottles of water and some apples. Which I had purchased on the way. Which happens to be water from the Devin province, which considering my ultimate purpose of the trip just seemed to make sense. He seemed very disappointed by that.

 |
| The Snail House |
 |
| Church of Saint John Rila/ Lada / Abandoned Bus Shelter |
 |
| The Woods at the foot of Vitosha |
I sit down. Read a little bit and write a bit more. Get to bed and fall asleep. The next day I packed everything up and headed back home. Happy.

Friday, 6 April 2018
Metal Nurse: Alcohol Free For The Year

Yes, I am not an alcoholic and I didn't feel like I am becoming one. But quite frankly I didn't want to risk becoming one. It just doesn't feel worth it. There isn't just the physical health side of things to consider there is also the mental health aspect of it. For many it is a form of coping mechanism to drink excessively, to suppress their depression and hide their anxiety. Without actually being aware that it is making both of those worse. Long-term excessive drinking can and does lead to psychosis and dementia. To go from wanting a drink to needing a drink, when you feel jittery and shaking, which doesn't stop until you've had your breakfast consisting of last nights unfinished booze. If you already suffer from depression/anxiety you run the risk of making it worse, and if you don't suffer from those debilitating illnesses you run the risk of developing them. Then there is the public health implication. In the UK excessive alcohol consumption costs society as a whole a whopping £21 billion. In the US the number is $249 billion, and that was in 2010, I can't imagine that that number has gone down since. WHO estimates that alcohol accounts for 5.1% of the total global disease burden, in 2012 over 3 million died due to alcohol-related conditions.

I know that there is also that rumour that it helps to relax, but I am not so sure anymore. I didn't actually find that it does. If anything I feel more stressed, especially the day after, my sleep is more disrupted and I am even grumpier when I wake up. All good research also shows that. You don't get enough sleep. You don't get enough REM sleep, it disrupts your circadian rhythm because alcohol relaxes your muscles it makes you more prone to sleep apnea, etc etc. Recent research have been implicating lack of sleep as one of the causes of ill mental health, as opposed to a symptom. So it all seems a little circular. I felt it was time to smash that circle. I like my sleep, and I prefer my sleep to be undisturbed. I especially didn't want to have to wake up several times just to have to empty my bladder. I want to wait at least another 50 years until that has to be a feature in my life.

Even just looking at the health evidence of all the ill effects that alcohol does to your body and mind. Alcohol has been linked to an increased risk of cancer development. At least 7 different ones, including breast cancer, bowel cancer and liver cancer. Drinking also increases your risk of developing cirrhosis of the liver, which itself is a risk factor in developing cancer of the liver. There is also increased the risk of developing acute pancreatitis, which itself leads to chronic pancreatitis, which in turn increases your risk of developing pancreatic cancer. Alcohol also adversely affects the cardiovascular system. It increases your risk of developing hypertension, coronary heart disease and peripheral vascular disease. All of which also increase your risk of stroke and heart attacks. You run the risk of developing Wernicke's Encephalopathy, which is caused by depletion of thiamine, this condition often precedes a condition called Korsakoff Syndrome. The more I read and the more I think about it, it just doesn't feel worth it.
Plus it's expensive. I don't particularly like the day after feeling, not just the full-blown hangover. But that 'bleurgh' feeling without a headache. Even without thinking about all the physical health issues, it just doesn't feel worth it. But giving up the alcohol. That does feel worth it.
Subscribe to:
Posts (Atom)